Is Overpronation
Overview
Over pronation is when there is excessive or too much movement of the foot. Over pronation is a very common cause of heel pain and general pain throughout the lower extremities. This condition can often be referred to as flat feet and causes you to walk on other parts of your foot, which is what leads to serious heel and foot pain.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
There are exercises that you can do to help deal with the effects and treat the cause. Obviously you can opt for an insert into your shoe either by way of your sports shop or go see a podiatrist. Like anything in your body that is not working correctly; you will have to manage your condition. Don't put off dealing with the problem as it will manifest associated issues along the alignment and as far up as your neck. If it's mild pronantion, I suggest running barefoot. If you can't do this then don't wear shoes at all at home or in the office as much as possible. Give your calf muscles a huge stretch everyday as these with the ligaments from the foot up to the muscle get tight and are linked to your pain. Loosen your calf muscles as much as possible. Great exercise is to sit barefoot with a marble on the floor in front of you. Grab the marble with your toes and try to hold it tight in the middle of the base of your foot. Ping pong balls and even golf balls work. Do this each night and combined with calf stretches you'll start to correct the muscle alignment gradually in the foot. Put more attention into massaging your feet, standing with a good posture, stretching your feet, ankles and calf muscles. Lastly, if you are fat this will not help at all. You must lose weight swimming, cycling and eradicating sugar and fat from your diet. The added strain on the foot by being a fat body compounds the problems and inhibits corrective results that you are after.
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
Over pronation is when there is excessive or too much movement of the foot. Over pronation is a very common cause of heel pain and general pain throughout the lower extremities. This condition can often be referred to as flat feet and causes you to walk on other parts of your foot, which is what leads to serious heel and foot pain.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
There are exercises that you can do to help deal with the effects and treat the cause. Obviously you can opt for an insert into your shoe either by way of your sports shop or go see a podiatrist. Like anything in your body that is not working correctly; you will have to manage your condition. Don't put off dealing with the problem as it will manifest associated issues along the alignment and as far up as your neck. If it's mild pronantion, I suggest running barefoot. If you can't do this then don't wear shoes at all at home or in the office as much as possible. Give your calf muscles a huge stretch everyday as these with the ligaments from the foot up to the muscle get tight and are linked to your pain. Loosen your calf muscles as much as possible. Great exercise is to sit barefoot with a marble on the floor in front of you. Grab the marble with your toes and try to hold it tight in the middle of the base of your foot. Ping pong balls and even golf balls work. Do this each night and combined with calf stretches you'll start to correct the muscle alignment gradually in the foot. Put more attention into massaging your feet, standing with a good posture, stretching your feet, ankles and calf muscles. Lastly, if you are fat this will not help at all. You must lose weight swimming, cycling and eradicating sugar and fat from your diet. The added strain on the foot by being a fat body compounds the problems and inhibits corrective results that you are after.
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
What Is Severs Disease?
Overview
Sever?s disease (also known as calcaneal apophysitis) is a type of bone injury in which the growth plate in the lower back of the heel, where the Achilles tendon (the heel cord that attaches to the growth plate) attaches, becomes inflamed and causes pain. Sever?s disease is the most common cause of heel pain in children, especially those who exercise or play sports on a regular basis.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The pain is at the heel or around the Achilles tendon. This is felt commonly during exercise, particularly activities involving running or jumping. The back of the heel may also be tender to touch and there may be localised swelling. There may be stiffness in the calf muscles first thing in the morning and you may notice limping or a tendency to tiptoe.
Diagnosis
A Podiatrist can easily evaluate your child?s feet, to identify if a problem exists. Through testing the muscular flexibility. If there is a problem, a treatment plan can be create to address the issue. At the initial treatment to control movement or to support the area we may use temporary padding and strapping and depending on how successful the treatment is, a long-term treatment plan will be arranged. This long-term treatment plan may or may not involve heel raises, foot supports, muscle strengthening and or stretching.
Non Surgical Treatment
To help relieve pain, give your child nonprescription pain medicine, such as acetaminophen, ibuprofen, or naproxen, as directed by your child?s provider. Nonsteroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen and naproxen, may cause stomach bleeding and other problems. Read the label and take as directed. Unless recommended by your healthcare provider, your child should not take the medicine for more than 10 days. Check with your healthcare provider before you give any medicine that contains aspirin or salicylates to a child or teen. This includes medicines like baby aspirin, some cold medicines, and Pepto-Bismol. Children and teens who take aspirin are at risk for a serious illness called Reye's syndrome. Ask your child?s healthcare provider, How and when you will hear your child?s test results. How long it will take for your child to recover. What activities your child should avoid and when your child can return to normal activities. How to take care of your child at home. What symptoms or problems you should watch for and what to do if your child has them. Make sure you know when your child should come back for a checkup.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Sever?s disease (also known as calcaneal apophysitis) is a type of bone injury in which the growth plate in the lower back of the heel, where the Achilles tendon (the heel cord that attaches to the growth plate) attaches, becomes inflamed and causes pain. Sever?s disease is the most common cause of heel pain in children, especially those who exercise or play sports on a regular basis.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The pain is at the heel or around the Achilles tendon. This is felt commonly during exercise, particularly activities involving running or jumping. The back of the heel may also be tender to touch and there may be localised swelling. There may be stiffness in the calf muscles first thing in the morning and you may notice limping or a tendency to tiptoe.
Diagnosis
A Podiatrist can easily evaluate your child?s feet, to identify if a problem exists. Through testing the muscular flexibility. If there is a problem, a treatment plan can be create to address the issue. At the initial treatment to control movement or to support the area we may use temporary padding and strapping and depending on how successful the treatment is, a long-term treatment plan will be arranged. This long-term treatment plan may or may not involve heel raises, foot supports, muscle strengthening and or stretching.
Non Surgical Treatment
To help relieve pain, give your child nonprescription pain medicine, such as acetaminophen, ibuprofen, or naproxen, as directed by your child?s provider. Nonsteroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen and naproxen, may cause stomach bleeding and other problems. Read the label and take as directed. Unless recommended by your healthcare provider, your child should not take the medicine for more than 10 days. Check with your healthcare provider before you give any medicine that contains aspirin or salicylates to a child or teen. This includes medicines like baby aspirin, some cold medicines, and Pepto-Bismol. Children and teens who take aspirin are at risk for a serious illness called Reye's syndrome. Ask your child?s healthcare provider, How and when you will hear your child?s test results. How long it will take for your child to recover. What activities your child should avoid and when your child can return to normal activities. How to take care of your child at home. What symptoms or problems you should watch for and what to do if your child has them. Make sure you know when your child should come back for a checkup.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
What Is The Cause Of Adult Aquired Flat Foot
Overview
Over 60 Million Americans suffer from Adult Acquired Flatfoot (AAF), otherwise known as Posterior Tibial Tendon Dysfunction or PTTD. This condition generally occurs in adults from 40-65 years of age, and it usually only occurs in one foot, not both. The Posterior Tibial (PT) Tendon courses along the inside part of the ankle and underneath the arch of the foot. It is the major supporting structure for the arch. Over time, the tendon becomes diseased, from overuse, and starts to lose it's strength. As a result, the arch begins to collapse, placing further strain on the PT Tendon, leading to further decrease in tendon strength, which causes further collapse of the arch. This is described as a progressive deformity because it will generally get worse over time. 
Causes
A person with flat feet has greater load placed on the posterior tibial tendon which is the main tendon unit supporting up the arch of the foot. Throughout life, aging leads to decreased strength of muscles, tendons and ligaments. The blood supply diminishes to tendons with aging as arteries narrow. Heavier, obese patients have more weight on the arch and have greater narrowing of arteries due to atherosclerosis. In some people, the posterior tibial tendon finally gives out or tears. This is not a sudden event in most cases. Rather, it is a slow, gradual stretching followed by inflammation and degeneration of the tendon. Once the posterior tibial tendon stretches, the ligaments of the arch stretch and tear. The bones of the arch then move out of position with body weight pressing down from above. The foot rotates inward at the ankle in a movement called pronation. The arch appears collapsed, and the heel bone is tilted to the inside. The deformity can progress until the foot literally dislocates outward from under the ankle joint.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Although AAF is not reversible without surgery, appropriate treatment should address the patient?s current symptoms, attempt to reduce pain, and allow continued ambulation. In the early stages, orthotic and pedorthic solutions can address the loss of integrity of the foot?s support structures, potentially inhibiting further destruction.3-5 As a general principle, orthotic devices should only block or limit painful or destructive motion without reducing or restricting normal motion or muscle function. Consequently, the treatment must match the stage of the deformity. 
Surgical Treatment
Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist.
Flat Feet In Adults
Overview
Adult acquired flatfoot deformity (AAFD or AAF) is a progressive, symptomatic deformity resulting from gradual stretch of the posterior tibial tendon as well as other ligaments supporting the arch of the foot. AAFD develops after skeletal maturity, May also be referred to as posterior tibial tendon dysfunction (PTTD), although due to the complexity of the disorder AAFD is more appropriate. Significant ligamentous rupture occurs as the deformity progresses. Involved ligaments include the spring ligament, the superficial deltoid ligament, the plantar fascia, and the long and short plantar ligaments. Unilateral AAFD is more common than bilateral AAFD.
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful. General components of the treatment include the use of comfort shoes. Activity modification to avoid exacerbating activities. Weight loss if indicated. Specific components of treatment that over time can lead to marked improvement in symptoms include a high repetition, low resistance strengthening program. Appropriate bracing or a medial longitudinal arch support. If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon complex can be successful. In stage 2 deformities, this is combined with an ankle brace for a period of 2-3 months until the symptoms resolve. At this point, the patient is transitioned to an orthotic insert which may help to support the arch. In patients with stage 1 deformity it may be possible to use an arch support immediately.

Surgical Treatment
Surgery should only be done if the pain does not get better after a few months of conservative treatment. The type of surgery depends on the stage of the PTTD disease. It it also dictated by where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. Some of the common surgeries include. Tenosynovectomy, removing the inflamed tendon sheath around the PTT. Tendon Transfer, to augment the function of the diseased posterior tibial tendon with a neighbouring tendon. Calcaneo-osteotomy, sometimes the heel bone needs to be corrected to get a better heel bone alignment. Fusion of the Joints, if osteoarthritis of the foot has set in, fusion of the joints may be necessary.
Adult acquired flatfoot deformity (AAFD or AAF) is a progressive, symptomatic deformity resulting from gradual stretch of the posterior tibial tendon as well as other ligaments supporting the arch of the foot. AAFD develops after skeletal maturity, May also be referred to as posterior tibial tendon dysfunction (PTTD), although due to the complexity of the disorder AAFD is more appropriate. Significant ligamentous rupture occurs as the deformity progresses. Involved ligaments include the spring ligament, the superficial deltoid ligament, the plantar fascia, and the long and short plantar ligaments. Unilateral AAFD is more common than bilateral AAFD.
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful. General components of the treatment include the use of comfort shoes. Activity modification to avoid exacerbating activities. Weight loss if indicated. Specific components of treatment that over time can lead to marked improvement in symptoms include a high repetition, low resistance strengthening program. Appropriate bracing or a medial longitudinal arch support. If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon complex can be successful. In stage 2 deformities, this is combined with an ankle brace for a period of 2-3 months until the symptoms resolve. At this point, the patient is transitioned to an orthotic insert which may help to support the arch. In patients with stage 1 deformity it may be possible to use an arch support immediately.
Surgical Treatment
Surgery should only be done if the pain does not get better after a few months of conservative treatment. The type of surgery depends on the stage of the PTTD disease. It it also dictated by where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. Some of the common surgeries include. Tenosynovectomy, removing the inflamed tendon sheath around the PTT. Tendon Transfer, to augment the function of the diseased posterior tibial tendon with a neighbouring tendon. Calcaneo-osteotomy, sometimes the heel bone needs to be corrected to get a better heel bone alignment. Fusion of the Joints, if osteoarthritis of the foot has set in, fusion of the joints may be necessary.
Coping With Achilles Tendinitis
Overview
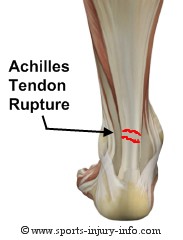 Your Achilles tendon is located at the back of your foot, just above your heel. It connects your heel to the two muscles of your calf and helps your foot push forward every time you take a step. If the tendon becomes swollen or irritated due to overuse, it can lead to the painful condition called Achilles tendonitis. If Achilles tendonitis goes untreated, it can become a chronic (ongoing) condition that makes just walking around almost impossible. Achilles tendonitis is a very common running injury. But it can also affect basketball players, dancers, or people who put a lot of repeated stress on their feet. It can be very painful.
Your Achilles tendon is located at the back of your foot, just above your heel. It connects your heel to the two muscles of your calf and helps your foot push forward every time you take a step. If the tendon becomes swollen or irritated due to overuse, it can lead to the painful condition called Achilles tendonitis. If Achilles tendonitis goes untreated, it can become a chronic (ongoing) condition that makes just walking around almost impossible. Achilles tendonitis is a very common running injury. But it can also affect basketball players, dancers, or people who put a lot of repeated stress on their feet. It can be very painful.
Causes
Tendinitis can result from an injury or over-use. Improper stretching prior to exertion or incorrect form during physical activity can also contribute to the development of tendinitis. Some people, including those with ?flat feet,? tight tendons or arthritis, are particularly prone to tendinitis.
Symptoms
Symptoms include pain in the heel and along the tendon when walking or running. The area may feel painful and stiff in the morning. The tendon may be painful to touch or move. The area may be swollen and warm. You may have trouble standing up on one toe.
Diagnosis
Your physiotherapist or sports doctor can usually confirm the diagnosis of Achilles tendonitis in the clinic. They will base their diagnosis on your history, symptom behaviour and clinical tests. Achilles tendons will often have a painful and prominent lump within the tendon. Further investigations include US scan or MRI. X-rays are of little use in the diagnosis.
Nonsurgical Treatment
Treatment for Achilles tendonitis, depends on the severity of the injury. If heel pain, tenderness, swelling, or discomfort in the back of the lower leg occurs, physical activity that produces the symptoms should be discontinued. If the problem returns or persists, a medical professional should be consulted. If pain develops even with proper stretching and training techniques, the patient should consult a podiatrist to check for hyperpronation and adequate arch support. The addition of an orthotic may be enough to maintain good arch and foot alignment and eliminate pain. If damage to the tendon is minor, the injury may respond to a simple course of treatment known as RICE (rest, ice, compression, elevation). Patients are advised to rest the tendon by keeping off their feet as much as possible, apply ice packs for 20 minutes at a time every hour for a day or two to reduce swelling, compress the ankle and foot with a firmly (not tightly) wrapped elastic bandage and elevate the foot whenever possible to minimize swelling. A nonsteroidal anti-inflammatory drug (NSAID) such as ibuprofen may be used to reduce pain, swelling, and inflammation.

Surgical Treatment
If non-surgical approaches fail to restore the tendon to its normal condition, surgery may be necessary. The foot and ankle surgeon will select the best procedure to repair the tendon, based upon the extent of the injury, the patient?s age and activity level, and other factors.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
Your Achilles tendon is located at the back of your foot, just above your heel. It connects your heel to the two muscles of your calf and helps your foot push forward every time you take a step. If the tendon becomes swollen or irritated due to overuse, it can lead to the painful condition called Achilles tendonitis. If Achilles tendonitis goes untreated, it can become a chronic (ongoing) condition that makes just walking around almost impossible. Achilles tendonitis is a very common running injury. But it can also affect basketball players, dancers, or people who put a lot of repeated stress on their feet. It can be very painful.
Causes
Tendinitis can result from an injury or over-use. Improper stretching prior to exertion or incorrect form during physical activity can also contribute to the development of tendinitis. Some people, including those with ?flat feet,? tight tendons or arthritis, are particularly prone to tendinitis.
Symptoms
Symptoms include pain in the heel and along the tendon when walking or running. The area may feel painful and stiff in the morning. The tendon may be painful to touch or move. The area may be swollen and warm. You may have trouble standing up on one toe.
Diagnosis
Your physiotherapist or sports doctor can usually confirm the diagnosis of Achilles tendonitis in the clinic. They will base their diagnosis on your history, symptom behaviour and clinical tests. Achilles tendons will often have a painful and prominent lump within the tendon. Further investigations include US scan or MRI. X-rays are of little use in the diagnosis.
Nonsurgical Treatment
Treatment for Achilles tendonitis, depends on the severity of the injury. If heel pain, tenderness, swelling, or discomfort in the back of the lower leg occurs, physical activity that produces the symptoms should be discontinued. If the problem returns or persists, a medical professional should be consulted. If pain develops even with proper stretching and training techniques, the patient should consult a podiatrist to check for hyperpronation and adequate arch support. The addition of an orthotic may be enough to maintain good arch and foot alignment and eliminate pain. If damage to the tendon is minor, the injury may respond to a simple course of treatment known as RICE (rest, ice, compression, elevation). Patients are advised to rest the tendon by keeping off their feet as much as possible, apply ice packs for 20 minutes at a time every hour for a day or two to reduce swelling, compress the ankle and foot with a firmly (not tightly) wrapped elastic bandage and elevate the foot whenever possible to minimize swelling. A nonsteroidal anti-inflammatory drug (NSAID) such as ibuprofen may be used to reduce pain, swelling, and inflammation.
Surgical Treatment
If non-surgical approaches fail to restore the tendon to its normal condition, surgery may be necessary. The foot and ankle surgeon will select the best procedure to repair the tendon, based upon the extent of the injury, the patient?s age and activity level, and other factors.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
What Exactly Causes Pain In The Heel

Overview
Do you have sharp, stabbing, and/or aching pain on the bottom of your heel or arch?
Is the pain more severe when you first get up in the morning or when you first start walking after rest? If this describes your pain then you probably suffer from a condition known as PLANTAR FASCIITIS. It sounds complicated, but plantar fasciitis is actually one of the most common foot problems. In the past plantar fasciitis has been called by other names, such as heel spur syndrome, bone spurs or a stone bruise on the heel. The plantar fascia is a long thick ligament that runs along the arch of your foot from your heel bone (the calcaneus) to the ball of the foot. The job of the plantar fascia is to help support your arch. When the fascia becomes inflamed and painful we call this PLANTAR FASCIITIS. The pain from plantar fasciitis most commonly occurs near the attachment of the fascia to the calcaneus (heel bone), which is why most people who suffer from plantar fasciitis have pain on the bottom or inside of the heel. However, the pain can be anywhere along the fascia from the heel to the ball of the foot.
Causes
There are several possible causes of plantar fasciitis, including wearing high heels, gaining weight, increased walking, standing, or stair-climbing. If you wear high-heeled shoes, including western-style boots, for long periods of time, the tough, tendonlike tissue of the bottom of your foot can become shorter. This layer of tissue is called fascia. Pain occurs when you stretch fascia that has shortened. This painful stretching might happen, for example, when you walk barefoot after getting out of bed in the morning. If you gain weight, you might be more likely to have plantar fasciitis, especially if you walk a lot or stand in shoes with poor heel cushioning. Normally there is a pad of fatty tissue under your heel bone. Weight gain might break down this fat pad and cause heel pain. Runners may get plantar fasciitis when they change their workout and increase their mileage or frequency of workouts. It can also occur with a change in exercise surface or terrain, or if your shoes are worn out and don't provide enough cushion for your heels. If the arches of your foot are abnormally high or low, you are more likely to develop plantar fasciitis than if your arches are normal.
Symptoms
The typical presentation is sharp pain localized at the anterior aspect of the calcaneus. Plantar fasciitis has a partial association with a heel spur (exostosis); however, many asymptomatic individuals have bony heel spurs, whereas many patients with plantar fasciitis do not have a spur.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
Treatment for plantar fasciitis includes medication, physical therapy, shock wave therapy, or surgery. Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen are used to treat the inflammation and pain of plantar fasciitis, but they won’t cure the condition. Corticosteroids can also be used to ease pain and reduce inflammation. Corticosteroids are applied either as a topical solution in conjunction with a non-painful electric current or through injections to the affected area.

Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
Stretching Exercises
Stretching your plantar fasciitis is something you can do at home to relieve pain and speed healing. Ice massage performed three to four times per day in 15 to 20 minute intervals is also something you can do to reduce inflammation and pain. Placing arch supports in your shoes absorbs shock and takes pressure off the plantar fascia.
What Is Pain At The Heel And Tips On How To Cure It

Overview
The Plantar Fascia is a broad, thick band of tissue that runs from under the heel to the front of the foot. Through overuse the fascia can become inflamed and painful at its attachment to the heel bone or calcaneus. The condition is traditionally thought to be inflammation, however this is now believed to be incorrect due to the absence of inflammatory cells within the fascia. The cause of pain is thought to be degeneration of the collagen fibres close to the attachment to the heel bone.
Causes
Although plantar fasciitis may result from a variety of factors, such as repeat hill workouts and/or tight calves, many sports specialists claim the most common cause for plantar fasciitis is fallen arches. The theory is that excessive lowering of the arch in flat-footed runners increases tension in the plantar fascia and overloads the attachment of the plantar fascia on the heel bone (i.e., the calcaneus). Over time, the repeated pulling of the plantar fascia associated with excessive arch lowering is thought to lead to chronic pain and inflammation at the plantar fascia’s attachment to the heel. In fact, the increased tension on the heel was believed to be so great that it was thought to eventually result in the formation of a heel spur.
Symptoms
Plantar fasciitis is the inflammation of the plantar fascia - a band of tough fibrous tissue running along the sole of the foot. It occurs when small tears develop in the plantar fascia, leading to inflammation and heel pain. The plantar fascia tissue branches out from the heel like a fan, connecting the heel bone to the base of the toes. When the foot moves, the plantar fascia stretches and contracts. The plantar fascia helps to maintain the arch of the foot in much the same way that the string of a bow maintains the bow's arch. The most notable symptom of plantar fasciitis is heel pain. This is typically most severe in the middle of the heel though it may radiate along the sole of the foot. The pain is most often felt when walking first thing in the morning or after a period of rest. As walking continues the pain may decrease; however some degree of pain remains present on movement. The pain may disappear when resting, as the plantar fascia is relaxed. Redness, swelling and warmth over the affected area may also be noticed. The onset of plantar fasciitis is gradual and only mild pain may be experienced initially. However, as the condition progresses the pain experienced tends to become more severe. Chronic plantar fasciitis may cause a person to change their walking or running action, leading to symptoms of discomfort in the knee, hip and back.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
Anti-inflammatory medications can help decrease the inflammation in the arch and heel of your foot. These medications include Advil, Mtrin, Ibuprofen, and Aleve. Use the medication as directed on the package. If you tolerate it well, take it daily for two weeks then discontinue for one week. If symptoms worsen or return, resume for two weeks, then stop. You should eat when taking these medications, as they can be hard on your stomach. Ach Support. Over the counter inserts provide added arch support and soft cushion. Based on the individual needs of your foot, you may require custom inserts. Achilles Tendon Stretch. Pace a shoe insert under your affected foot. Place your affected leg behind your unaffected leg with the toes of your back foot pointed towards the heel of your other foot. Lean into the wall. Bend your front knee while keeping your back leg straight with your heel firmly on the ground. Hold the stretch for a count of 10. A set is 10 repetitions. Perform the stretch at least three times a day.

Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints, a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as, open surgery, where the section of the plantar fascia is released by making a cut into your heel, endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to, have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention
Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.